Article Text

Abstract
BACKGROUND Historical cohort studies in England have found that impaired fetal growth and lower respiratory tract infections in early childhood are associated with lower levels of lung function in late adult life. These relations are investigated in a similar study in Scotland.
METHODS In 1985–86 a follow up study was carried out of 1070 children who had been born in St Andrew’s from 1921 to 1935 and followed from birth to 14 years of age by the Mackenzie Institute for Medical Research. Recorded information included birth weight and respiratory illnesses. The lung function of 239 of these individuals was measured.
RESULTS There was no association between birth weight and lung function. Pneumonia before two years of age was associated with a difference in mean forced expiratory volume in one second (FEV1) of −0.39 litres (95% confidence interval (CI) −0.67, −0.11; p = 0.007) and in mean forced vital capacity (FVC) of −0.60 litres (95% CI −0.92, −0.28; p<0.001), after controlling for age, sex, height, smoking, type of spirometer, and other illnesses before two years. Similar reductions were seen in men and women. Bronchitis before two years was associated with smaller deficits in FEV1 and FVC. Asthma or wheeze at two years and older and cough after five years were also associated with a reduction in FEV1.
CONCLUSIONS The relation between impaired fetal growth and lower lung function in late adult life seen in previous studies was not confirmed in this cohort. The deficits in FEV1 and FVC associated with pneumonia and bronchitis in the first two years of life are consistent with a causal relation.
- childhood pneumonia
- birth weight
- adult lung function
Statistics from Altmetric.com
It has been proposed that impaired lung growth may lead to chronic airflow obstruction in late adult life through a failure to attain maximal lung function potential as a young adult, even if the subsequent rate of decline with age is normal.1 Studies of children have suggested that fetal growth retardation and lower respiratory tract infection (LRTI) in early childhood may be important risk factors for impaired lung growth. Lower birth weight for a given gestational age,2 and a history of bronchitis, pneumonia, and bronchiolitis3-7 have been associated with lower lung function.
To investigate the relations of fetal growth retardation and childhood LRTI to lung function in late adult life it is necessary to follow up individuals, for whom information about birth weight and LRTI has been collected in early childhood, for 60 years or more. An ongoing prospective study of individuals born 50 years ago in Britain may provide important answers in the future.8 An alternative approach is to identify individuals in late adult life for whom detailed records of child health are available. A historical cohort study of men born from 1911 to 1930 in Hertfordshire showed that men who were lighter at birth, and who had had bronchitis, pneumonia or whooping cough in infancy, had lower lung function than other men, after controlling for age, height, smoking, and social class.9 A similar study of men and women born from 1917 to 1922 in Derbyshire showed that pneumonia before two years of age was associated with a large reduction in lung function in men but not in women; however, no deficit associated with bronchitis or whooping cough was found.10
The opportunity arose to examine the relations of birth weight and childhood LRTI to adult lung function in a cohort of men and women born from 1921 to 1935 in Scotland. Previous analyses in this cohort had shown that adults with chronic bronchitis were more likely to have had “chronic catarrh” documented in childhood.11-13
Methods
In 1919 the Mackenzie Institute for Clinical Research was founded in St Andrews, Scotland. Detailed records of child health were kept in a standardised form by the doctor in charge of the children’s department. The institute’s records contained information about the growth of children and the illnesses they had experienced from birth until 14 years of age. This was documented during the first two years of life by the Child Welfare Clinic and subsequently by the institute which invited children to attend three times a year from 2 to 5 years of age and annually thereafter. At each visit mothers were interviewed about their child’s health and asked to report any illnesses and the age at illness. If the general practitioner had been consulted the diagnosis was used as confirmation of the report. Respiratory illnesses included cough, bronchitis, pneumonia, wheeze, asthma, whooping cough, measles, croup, and influenza. Other information in the records included birth weight and father’s occupation. There was no quantitative information on gestational age but births were recorded as “full term” or “premature”.
In 1985–86 a follow up study was carried out of 1070 people who had attended the Mackenzie Institute as children to investigate the relation between childhood respiratory illness and adult respiratory disease. This sample comprised 70% of all children born in the Burgh of St Andrews in 1921 to 193512 ,13 and included children with sufficient information from the Mackenzie records for follow up. Details of the tracing methods have been reported previously.12 The status of the study sample in 1986 is shown in fig 1. A total of 653 individuals (61%) were still alive and traced, and 183 individuals had died. Of these deaths, 107 (58%) had occurred in the first five years of life, of which 22 were attributed to pneumonia, bronchopneumonia, and bronchitis, and 55 (30%) had occurred after 40 years of age, of which five were attributed to chronic bronchitis, emphysema, and asthma.

Follow up of Mackenzie cohort.
The 653 traced individuals were mailed a questionnaire that asked about respiratory symptoms and smoking history,14occupation and education, and parents’ smoking history. A total of 468 (72%) individuals responded. Of the questionnaire responders, 414 were still living in St Andrew’s or other parts of Fife and Tayside, and they were invited to have their lung function measured. Spirometry was performed with the subjects standing and, after practice blows, five forced expiratory manoeuvres were recorded. Lung function was measured using either a Vitalograph spirometer (Vitalograph Ltd., Buckingham, UK) at a clinic or a turbine spirometer at home; the latter instrument was used for all subjects who did not live in the immediate vicinity of Dundee or St Andrew’s (58%). Field workers were blind to the contents of the child health records.
Each of the respiratory illnesses was categorised according to whether it had been experienced before 2 years of age, between 2 and 5 years, or after 5 years. The cut off of 2 years was chosen a priori for comparability with previous studies.4 ,8 ,10Bronchopneumonia, and measles or influenza accompanied by pneumonia, were included under the diagnosis of “pneumonia”. “Asthma” and “wheeze” were combined as one entity. Children were classified as “atopic” if they had a history of hay fever, eczema, or allergic urticaria. Social class at birth was classified according to the Registrar General’s classification15 using information on father’s occupation. Occupational and educational histories were used to classify adult social class as manual and non-manual in the same way. Women’s social class was based on their own occupation if they lived alone, otherwise on their partner’s occupation.
Lung function data were analysed by multiple linear regression using Stata.16 The highest values of forced expiratory volume in one second (FEV1) and forced vital capacity (FVC) from satisfactory manoeuvres were used in the analysis even if they came from different blows.17 Main analyses controlled for age, sex, height, smoking, and type of spirometer. Lifetime smoking history was expressed as a categorical variable (never, exsmoker, and current smoker) and in smokers as a continuous variable (pack-years). Both smoking variables were included in the regression analyses18; we found that square root of pack years had a linear association with FEV1 and FVC and therefore this was used in the analyses. We tested for interactions between sex and age, height and smoking on lung function. Subsidiary analyses also controlled for social class at birth, adult social class, maternal smoking, paternal smoking, and atopy.
Results
Among the questionnaire responders 243 agreed to spirometric testing; 128 men and 112 women performed satisfactorily. We examined characteristics of individuals from the original study sample according to their tracing status in 1986, whether they had responded to the questionnaire and whether lung function data had been obtained. There was no difference in mean birth weight or in the prevalence of childhood respiratory morbidity between those individuals from the original study sample who were traced and untraced or between questionnaire responders and non-responders. Also, mean birth weight was similar between those alive and those who had died. Among the questionnaire responders, individuals with lung function data had a similar mean birth weight to those without, but were significantly more likely to be smokers and to be of manual social class.
The mean (SD) age of the subjects was 57.6 (4.3) years. The difference between the highest and second highest FEV1 was ⩽0.2 litres in 95% of subjects; 93% achieved a similar reproducibility for FVC.17 Mean (SD) unadjusted FEV1 and FVC were, respectively, 2.99 (0.64) litres and 4.19 (0.74) litres in men, and 2.30 (0.46) litres and 3.06 (0.54) litres in women. We found a highly significant interaction between sex and age on FEV1 and FVC; 34% of men and 24% of women had smoked in the past, and 44% and 34%, respectively, were still smoking. The main analyses were restricted to 239 individuals with complete information.
Mean (SD) birth weight was 3.41 (0.55) kg. Birth weight was unrelated to lung function. After controlling for age, sex, height, smoking, and type of spirometer, estimated changes in FEV1 and FVC, per change in birth weight (litres/kg) were, respectively, 0.036 (95% confidence interval (CI) −0.074, 0.147; p = 0.52) and 0.010 (95% CI −0.119, 0.139; p = 0.88). Fifteen children (6%) were born “prematurely”. Controlling for prematurity did not alter the findings for birth weight.
Table 1 shows the differences in mean lung function associated with different types of LRTI before 2 years of age, after controlling for age, sex, height, smoking, type of spirometer, and other illnesses listed in the table. Pneumonia before 2 years was associated with a reduction in mean FEV1 (difference −0.39 litres (95% CI −0.67, −0.11; p = 0.007) and in mean FVC (difference −0.60 litres (95% CI −0.92, −0.28; p<0.001) but not in mean FEV1/FVC. The effect of pneumonia before 2 years on lung function was similar in men and women (mean difference in FEV1 −0.38 litres (95% CI −0.81, 0.06) and −0.34 litres (95% CI −0.68, −0.002)), respectively. Bronchitis before 2 years was also associated with lower lung function, although the reductions were smaller (mean difference in FEV1 −0.13 litres (95% CI, −0.25, −0.001) and mean difference in FVC −0.15 litres (95% CI −0.30, −0.01)). The effects of pneumonia and bronchitis before 2 years on FEV1 and FVC were little altered by further controlling for illnesses after 2 years of age, social class at birth, current social class, maternal smoking, paternal smoking, and atopy. Whooping cough and other illnesses before 2 years were not associated with lower lung function.
Difference in mean lung function (95% CI)1-150 associated with different respiratory illnesses before 2 years of age in 239 men and women
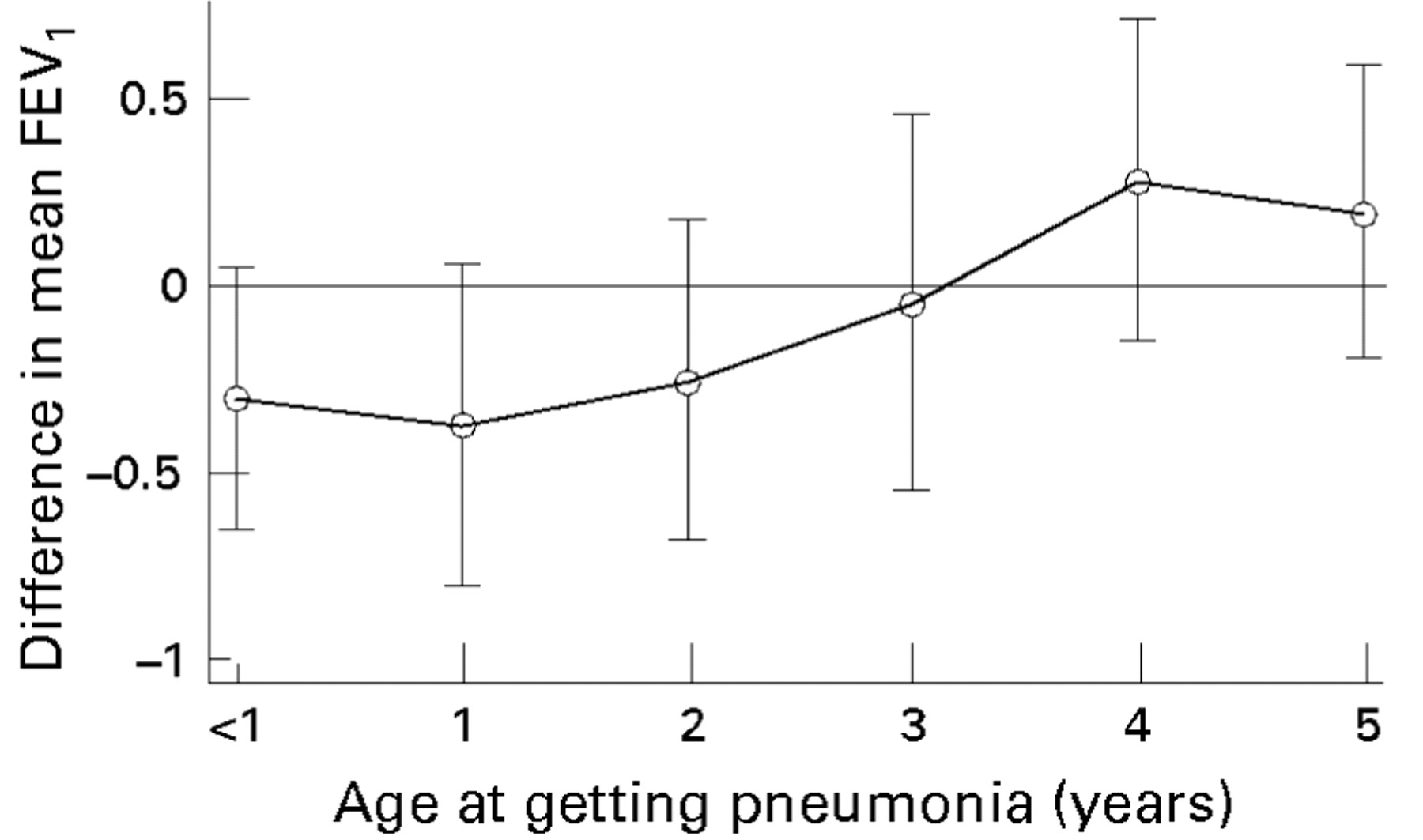
Pneumonia and bronchitis at 2 years of age and older were not associated with a reduction in lung function. However, asthma or wheeze at 2 years and older, and cough after 5 years, were associated with reductions in FEV1 (table 2). We examined the relation between age at getting pneumonia and FEV1 in one year intervals (fig 2). This suggested that pneumonia was associated with a reduction in FEV1 until 3 years of age.
Difference in mean lung function (95% CI)2-150 associated with different respiratory illnesses at 2 years of age and older in 239 men and women
{kind=link}
{kind=link}
Relation between difference (95% CI) in mean FEV1 and age at getting pneumonia (controlling for age, sex, height, smoking history, and type of spirometer).
Discussion
This study has shown that pneumonia and bronchitis in the first 2 years of life were associated with a lower level of FEV1and FVC in late middle age. Other illnesses before 2 years of age, including whooping cough, were not associated with impaired lung function, but in later childhood asthma or wheeze and cough were associated with reductions in FEV1. No association was found between birth weight and lung function.
In this follow up study, questionnaire and lung function data were obtained from only 44% and 22%, respectively, of the original study sample (fig 1). It is therefore important to consider whether our findings could have been biased through losses to follow up of the individuals who were untraced, those who had died before 1986, those who did not respond to the questionnaire or those for whom lung function data were not obtained. We cannot exclude this possibility. However, questionnaire responders and those agreeing to spirometry appeared to be representative of the original study sample with respect to birth weight and childhood respiratory illness. Furthermore, if the main finding had arisen through selection bias, then pneumonia in early childhood would have to be associated with better lung function in those individuals in the original study sample for whom lung function data were not obtained, which seems unlikely.
We found no relation between birth weight and lung function. This is in contrast to the findings of two historical cohort studies from England9 and India.19 A study of children, with information on gestational age, confirmed that the association between lower birth weight and lower lung function was a consequence of impaired fetal growth rather than prematurity.2 While we did not have quantitative information on gestational age, controlling for “premature” birth did not alter our findings. It is possible, however, that our effect estimates differ as a consequence of sampling variation; the lower 95% confidence interval for the coefficient of birth weight on FEV1 in our study overlapped with the upper limit for the coefficients in the other two studies.
In this study we were testing, a priori, the hypotheses that bronchitis, pneumonia, and whooping cough before 2 years of age are associated with reduced lung function in late adult life. Given this, and the level of significance for the associations between early pneumonia and FEV1 and FVC (p = 0.007 and p<0.001, respectively), we think it unlikely that our findings for pneumonia, at least, arose through chance. The evidence for an association with bronchitis, however, is less strong.
An important potential confounder to consider is maternal smoking in pregnancy. This is associated with a higher incidence of respiratory infections,20 and with lower lung function21in infancy, although a link between maternal smoking and lower lung function in adult life has not been reported. We found that maternal smoking, reported by 23% of subjects, was not related to adult lung function and did not therefore confound the pneumonia effect. While our information on maternal smoking was based on recall and could not distinguish maternal smoking in pregnancy from that in childhood, a recent study with more reliable information on maternal smoking in pregnancy confirmed that this exposure did not confound the association between childhood pneumonia and adult lung function.22
The reduction in FEV1 and FVC associated with pneumonia and bronchitis before 2 years of age is consistent with a previous study of elderly men born in Hertfordshire in which pneumonia or bronchitis in infancy was associated with lower lung function in late adult life.9 A study of elderly men and women born in Derbyshire found that pneumonia, but not bronchitis, before 2 years was associated with a reduction in FEV1 and FVC in men, although the effect was smaller and non-significant in women.10 The lack of a reduction in the ratio FEV1/FVC was in keeping with one of these studies,9 ,23 but not the other.10 A recent study of the 1958 British national birth cohort found an association between pneumonia before 7 years of age and lower lung function in young adults.22 In that study the finding was independent of a history of asthma and wheezing and, as with our study, FEV1/FVC was normal, suggesting that childhood pneumonia is associated with smaller lung volumes but not with airflow obstruction.
What did “pneumonia” and “bronchitis” before 2 years of age represent? “Pneumonia” clearly represented a severe LRTI as it accounted for a substantial proportion of deaths under 5 years of age in this cohort.12 Furthermore, most childhood deaths from pneumonia occurred before 2 years of age. “Bronchitis” is likely to have been a less severe illness as it accounted for much fewer deaths and was associated with smaller reductions in lung function. Some of the cases of “pneumonia” and “bronchitis” before 2 years may have included what would be described today as “bronchiolitis”, a term not used in the 1920s. Interestingly, “cough” seemed to represent a different type of illness, as in later childhood, but not earlier, it was associated with an obstructive deficit in lung function. Cough at this later age and wheeze at 2 years and older may have been manifestations of asthma.
There are two possible interpretations of our findings. Either pneumonia and bronchitis in early childhood contributed to impairment of adult lung function, or individuals who experienced these illnesses already had lower lung function from birth. The latter possibility can only be addressed in prospective studies from birth to adult life in which neonatal lung function is measured before the occurrence of severe LRTI. While we cannot exclude this explanation, the substantial deficits in lung function associated with these illnesses are in keeping with a causal interpretation. The deficit in FEV1associated with pneumonia was greater than that associated with being a current smoker in this cohort.
How might early pneumonia and bronchitis have led to impaired adult lung function? The most likely explanation is that these illnesses had a deleterious effect on lung growth, which led to a failure to achieve maximal lung function potential in adult life. The lack of an obstructive deficit suggests that growth of the airways and the parenchyma were affected proportionately. Bronchitis and pneumonia in early childhood have been associated with impaired lung function in children.3 ,5 ,7 Gold and colleagues showed that boys with a history of pneumonia in the first 2 years of life subsequently had a slower rate of growth of lung function than other boys.4Retrospective studies of children have also found deficits in lung function associated with bronchiolitis.3 ,5 ,6 In animals viral pneumonia and bronchiolitis can interfere with lung growth.24 Pathological and radiological studies of children have shown that pneumonia caused by particular types of adenovirus can damage the lung, leading to bronchiolar obliteration and bronchiectasis, particularly if the illness occurs before 2 years of age.25-27 Furthermore, follow up later in childhood suggests that this damage is permanent and associated with impaired lung function.7 ,28
Although we had limited power to analyse the effect of pneumonia according to the year of life of illness, our findings suggest that the detrimental effect on adult lung function was restricted to the first 2 to 3 years of life and not beyond. This may be a critical period because of host factors (small size of the peripheral airways, fast rate of lung growth, immaturity of the immune system), the type of organism, and the size of infecting dose, which is larger in younger children who are more intensively exposed within the home. In contrast, in the 1958 national birth cohort the effect of pneumonia was no greater for those individuals who had pneumonia before 2 years than for those who had it between 2 and 7 years,22 although the history of early pneumonia was obtained retrospectively when the child was 7 years old.
Whooping cough was not associated with impaired lung function. This is consistent with the findings of most studies of children, adolescents and adults,10 ,29-32 but not all.9 ,22 ,33The lack of a reduction in lung function associated with measles is consistent with historical cohort studies from England,9 ,10 and from Guinea-Bissau, West Africa, where measles infection is severe (unpublished observations, S. Shaheen, 1995).
What are the public health implications of our findings? Pneumonia and bronchitis before 2 years of age were associated with substantial reductions in lung volumes. FEV1 is a strong predictor of mortality from chronic obstructive pulmonary disease (COPD).34 Thus, the decline in the incidence and severity of LRTI in early childhood which has occurred since the turn of the century in Britain may have contributed to the fall in mortality from COPD, which has been observed in recent decades in Britain,35 a trend that cannot be adequately explained by patterns of smoking.36 This is supported by an ecological study that showed a strong and very specific geographical correlation between infant mortality from pneumonia and bronchitis, and mortality from COPD in England and Wales 50 years later.37 For babies born today, however, our findings may be of greater importance in developing countries, where severe LRTI is still a leading cause of morbidity and mortality in young children.38 The impact of childhood LRTI on adult lung function needs to be evaluated in such a setting.
Acknowledgments
SOS and JACS are supported by the Department of Health, UK. The original data transcription and other data collection and analysis were supported by the Manpower Services Commission, The Wellcome Foundation, the Chief Scientist Organisation of the Scottish Home and Health Department and the MRC Environmental Epidemiology Unit, Southampton. We are grateful to Roberto Rona and Deborah Jarvis for helpful comments on an earlier version of this paper.