Article Text

Abstract
BACKGROUND Topical amethocaine provides effective pain relief during venepuncture in children, and has been shown to have a local anaesthetic action in the newborn.
AIM To investigate the effect of topical amethocaine on the pain of venepuncture in the newborn.
DESIGN Randomised double blind placebo controlled trial.
SUBJECTS Forty newborn infants, gestation 27–41 weeks (median 33), age 2–17 days (median 7), undergoing routine venepuncture.
METHOD A 1.5 g portion of 4% (w/w) amethocaine gel (Ametop; Smith and Nephew, Hull, UK) or placebo was applied to the skin under occlusion for one hour, then wiped away. Venepuncture was performed five minutes later. Facial reaction and cry were recorded on videotape. Pain was assessed using a validated adaptation of the neonatal facial coding system. Five features were scored at one second intervals for five seconds before and after venepuncture. No or minimal pain was defined as a cumulative score of below 10 (out of 25) in the five seconds after needle insertion. Each author scored the tapes independently.
RESULTS There was close agreement on scoring of the tapes. One infant was excluded because of restlessness before the venepuncture. Of 19 amethocaine treated infants, 16 (84%) showed little or no pain compared with six of 20 (30%) in the placebo group (p = 0.001). The median cumulative neonatal facial coding system score over five seconds after needle insertion was 3 compared with 16 in the placebo group (p = 0.001). Of the 19 amethocaine treated infants, 15 (79%) did not cry compared with five of 20 (25%) placebo treated infants (p = 0.001). No local reaction to amethocaine was seen.
CONCLUSION Topical amethocaine provides effective pain relief during venepuncture in the newborn.
- amethocaine
- anaesthetic
- pain
- venepuncture
Statistics from Altmetric.com
Painful invasive procedures are commonplace in the care of the newborn infant.1 One of the most frequently performed is venepuncture. In children, topical local anaesthetics are widely and successfully used before venepuncture to reduce or abolish the pain but their use has been less successful in the newborn infant. A lignocaine/prilocaine mixture (EMLA) which is effective in children has proved disappointing in the newborn.2 ,3 An effective topical local anaesthetic would be a useful tool in the management of procedural pain in the newborn.
Amethocaine is an ester group local anaesthetic available as a topical 4% (w/w) gel (Ametop). In several large studies in children, it has been shown to provide effective and safe local anaesthesia before venepuncture and intravenous cannulation.4-7 Using the cutaneous withdrawal reflex to assess anaesthesia, we have previously shown that topical amethocaine gel has a local anaesthetic action in the newborn infant that lasts for up to five hours.8 ,9 In the present study, we have assessed its ability to reduce the pain of venepuncture in the newborn infant.
Methods
We conducted a randomised double blind placebo controlled trial to investigate the effect of topical amethocaine gel on the pain of venepuncture in the newborn infant. We assessed pain in response to needle insertion using a validated adaptation of the neonatal facial coding system (NFCS) and by the presence and length of crying.10 The adapted NFCS assesses each of the following facial characteristics as present (1 point) or absent (no points): eye squeeze, brow bulge, open mouth, deepened nasolabial folds, and cry. Independent assessors scored the presence or absence of each of these features for each subject. In addition, we recorded the total length of cry in response to the needle, defined as a cry starting within five seconds of needle insertion and finishing with a gap of at least 30 seconds before any further cry. A Sony CCD-F450E Handycam in long play mode at a tape speed of 0.25 seconds per frame was used to record and play back the videotapes.
Infants who needed a venepuncture as part of their routine care were recruited for the study. A suitable vein for blood sampling was identified on the dorsum of the hand or foot. Then 1.5 g 4% (w/w) amethocaine gel or 1.5 g placebo was applied. The placebo was identical in every way except for the absence of the amethocaine component. The gel was covered with an occlusive dressing (Tegaderm, 3M Healthcare, Barben, Germany) and left alone. After one hour, the occlusive dressing was removed and the excess gel wiped away. The baby was left to settle for five minutes. Venepuncture was performed by one of a number of neonatal senior house officers with a range of experience in paediatrics from three to 24 months, or by an advanced neonatal nurse practitioner. There was no selection of personnel. Blood was taken for routine measurement of haematological and biochemical variables, requiring an average volume of 1.5 ml. A 21-ST needle (Butterfly; Abbott Ireland, Sligo, Republic of Ireland) was used for venepuncture and the exact moment that the needle pierced the skin was identified orally on the tape. The period from 20 seconds before needle insertion until the end of the cry was recorded. The two authors viewed the videotapes separately and independently. They assigned an NFCS score for each second, starting five seconds before the needle insertion and ending five seconds after needle insertion (giving a maximum cumulative score of 25 for each five second period). We defined a cumulative NFCS score of 10 or less in the five seconds after insertion of the needle as indicating no or minimal pain. The total length of the cry and its presence or absence over the five second period immediately after venepuncture were measured separately from the tapes. We measured the success of venepuncture by noting the number of attempts required to obtain the blood sample. This was defined as either one or more than one attempt.
SUBJECTS
We studied 40 unselected newborn infants from 27 to 41 weeks gestation (median 33) at 2–17 days of age (median 7). Infants admitted to the postnatal wards or neonatal intensive care unit at Nottingham City Hospital were eligible for entry but we excluded those who were unwell, ventilated, or sedated. The study was approved by the hospital's research ethics committee. Infants were studied with the informed written consent of the parent(s). We obtained exemption from the restrictions of the product licence of the drug from the Medicines Control Agency.
RANDOMISATION
Infants were randomised to have amethocaine or placebo gel applied to the venepuncture site. Randomisation was stratified within three gestational age groups: term, 33–36 weeks, and less than 33 weeks. The gels were packaged in identical tubes by the hospital pharmacy who randomised and coded them. The code was only broken at the end of the study after the videotapes had been scored and when the method of defining a painful or non-painful response had been agreed on.
STATISTICAL ANALYSIS
Statistical analysis was performed using SPSS 8.0 software. Tests for normality showed that the data were not normally distributed. The degree of agreement between the assessors in their scoring of the tapes was calculated using the facial action coding system reliability formula11:  The proportion of subjects in each group who showed no or minimal painful reaction to venepuncture and the proportion who cried were compared using Fisher's exact test. The cumulative NFCS values over five seconds after venepuncture and the total length of cry were compared by Mann-Whitney U testing for the amethocaine and placebo groups.
The proportion of subjects in each group who showed no or minimal painful reaction to venepuncture and the proportion who cried were compared using Fisher's exact test. The cumulative NFCS values over five seconds after venepuncture and the total length of cry were compared by Mann-Whitney U testing for the amethocaine and placebo groups.
Results
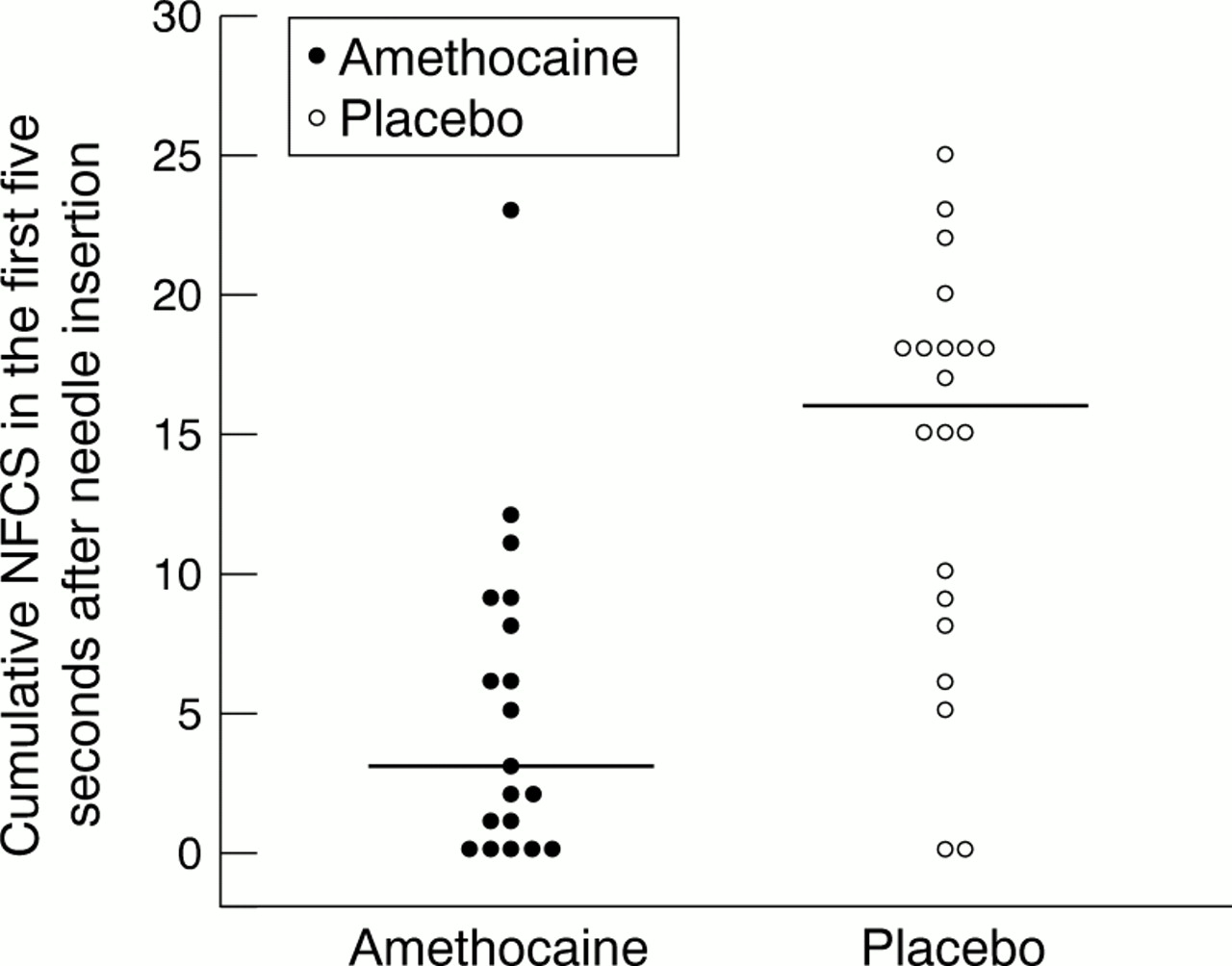
There were no significant differences in the characteristics of the infants in the two groups (table 1). For each feature of the NFCS, the coefficient of reliability between assessors was 0.96, 0.96, 0.94, 0.95, and 1.0 for eye squeeze, brow bulge, deepened nasolabial folds, open mouth, and cry respectively. One infant (amethocaine treated) was excluded from analysis before the code was broken because of restlessness before the venepuncture. In the five seconds immediately before needle insertion, the cumulative NFCS scores were not significantly different in the two groups (2 (0–5)v 0 (0–6) for amethocaine and placebo respectively; median (interquartile range (IQR))). In all, 16 of 19 (84%) amethocaine treated infants showed little or no pain in response to insertion of the needle compared with six of 20 (30%) in the placebo group (p = 0.001). The median cumulative NFCS score over the five seconds after needle insertion was 3 (IQR 0–9) in the amethocaine group compared with 16 (IQR 8–18) in the placebo group (p = 0.001) (fig 1). Logistic regression indicated that the cumulative NFCS score over five seconds before venepuncture did not influence the response to venepuncture. Fifteen of 19 (79%) in the amethocaine treated group compared with five of 20 (25%) in the placebo treated group did not cry at all in the five seconds immediately after needle insertion (p = 0.001). In those who did cry, the median total length of cry was 33 seconds (range 9–79) in the amethocaine group (n = 4) compared with 68 seconds (range 9–122) in the placebo treated group (n = 15). This twofold difference was not statistically significant. Fifteen of 19 (79%) samples were collected at the first attempt in the amethocaine group compared with 13 of 20 (65%) in the placebo group. This difference was not statistically significant. No local skin reactions were seen after application of amethocaine or placebo.
Details of groups of infants having amethocaine or placebo applied before venepuncture

{kind=link}
Cumulative neonatal facial coding system (NFCS) in the five seconds after needle insertion in infants treated with amethocaine or placebo. Horizontal bars indicate the median value in each group.
Discussion
In children and adults, topical local anaesthetics have been shown to provide safe and effective anaesthesia for a number of invasive procedures. In the newborn infant, their use has been less successful. Lignocaine and a lignocaine/prilocaine mixture (EMLA) have no demonstrable effect on the pain of heelprick.12-16Gourrier et al 17 reported a positive benefit of EMLA during venous and arterial puncture, although the study was open, uncontrolled, and non-randomised. Some 57% of EMLA treated infants compared with 18% of untreated infants showed a “weak” reaction to venous or arterial puncture. Acharyaet al 2 studied 19 preterm infants in a cross-over trial comparing EMLA with placebo. Using a combination of the NFCS and physiological variables to assess pain, they could show no effect of EMLA. Larsson et al 3 used the NFCS to assess pain of venepuncture in a similar study of 120 term infants. They found a statistically significant difference in the median pain scores after needle insertion and a reduction in the duration of cry in the EMLA treated group. However, the effect was a modest one.
Amethocaine as a 4% (w/w) gel (Ametop) has been developed for use as a topical local anaesthetic by McCafferty et al.18 It is licensed for use in term infants over 1 month of age. Structurally it has a lipophilic benzene ring attached to a tertiary amine group by an ester link chain. This differs from local anaesthetics such as lignocaine and prilocaine, which have an amide link chain. It acts by blocking the influx of sodium ions across the axon and thus the propagation of the action potential along the nerve. It is rapidly metabolised in the blood by plasma pseudocholinesterase. The plasma concentration of amethocaine and its metabolites was found to be unrecordable in seven of 10 adult subjects. In those in whom amethocaine was detected, no significant side effects were reported.19 Amethocaine for pain relief of venepuncture has been examined in three studies in children4-6 and found to be very effective. Transient erythema is common because of its vasodilator effect, in contrast with the pallor of vasoconstriction produced by EMLA.
There are no data on the clinical effectiveness of amethocaine in the newborn. In a pilot study of 20 healthy preterm infants using 1% amethocaine ointment, some evidence of percutaneous absorption was shown, with an increase in local skin blood flow, but local anaesthetic action was not assessed.20 We have shown, using the cutaneous withdrawal reflex to assess local anaesthesia, that amethocaine has a significant local anaesthetic action in the term and preterm newborn.9 The effect is detectable 30 minutes after application and lasts for up to five hours.8 A longer application time of 60 minutes results in a longer duration of action.
In this study we have shown that topical amethocaine gel has a very pronounced effect on the behavioural response of term and preterm infants to venepuncture. The effect is similar in magnitude to the reduction in pain score which has been found in studies of amethocaine gel in children. There were three amethocaine treatment failures. In one infant, the cumulative NFCS score over five seconds was 12 before venepuncture and 11 after, a treatment failure by our predetermined definition but clearly a treatment success. In another infant, the cumulative NFCS scores before and after venepuncture were 8 and 14 respectively, indicating some degree of anaesthesia. In the third infant, amethocaine had no anaesthetic effect at all. Fewer babies in the amethocaine treated group cried in the first five seconds after needle insertion, and in those who did, the total duration of cry was shorter. We deliberately chose not to use a single trained doctor or nurse to perform the venepuncture, as others have done, because we wanted the study conditions to represent the normal working practice of a neonatal unit.
The scoring system we used assesses the four most frequently occurring facial actions in response to an invasive stimulus, plus the presence or absence of crying.10 It is a modification of Grunau's original NFCS which was based on nine facial characteristics.21 ,22 The score has been validated as a tool for measuring procedural pain in the newborn10 and used for this purpose.16 The four facial actions and the cry could be clearly seen and heard on the video recordings. We found excellent agreement between the two assessors of the tapes on all five features.
Information is available on the safety of topical amethocaine gel in children but not in the newborn. Localised transient erythema occurs with a reported incidence of 6–24%. Local pruritus and oedema are less common. In our own experience, we have now applied topical amethocaine gel to 122 newborn infants from 27 to 42 weeks gestation. We have seen two instances of localised and transient erythema. In the current study, we did not observe any adverse reactions. There is no information on the metabolism of amethocaine in the newborn. It has been used in injected form in much higher doses than the topical preparation to provide regional anaesthesia in the newborn, without adverse effect.23 However, prolonged application of amethocaine gel for longer than one hour, repeated applications in a short period of time, and use in the very immature infant in the immediate newborn period should be avoided until more is known about its metabolism.
We conclude that topical amethocaine gel is highly effective in reducing the pain associated with venepuncture in the newborn infant. Further studies to assess its effect on other invasive procedures are needed.
Acknowledgments
This study was entirely funded by the Higher Education Funding Council. We are grateful to Dr Dermot McCafferty of Queen's University Belfast, who supplied the placebo gel, and to Sarah Pacey and Sarah Charlesworth of Nottingham City Hospital Pharmacy, who packaged the gels and carried out the randomisation and coding.
References
Linked Articles
- Original article