Article Text

Abstract
Aim: To evaluate the efficacy of silver iontophoretic central venous catheters in preventing catheter related colonisation and bloodstream infection among high risk patients in a tertiary hospital.
Methods: Patients requiring central venous access for a period greater than seven days were stratified into two groups according to systemic inflammatory response syndrome criteria before being randomly assigned to receive either silver iontophoretic or control catheters. The incidence of catheter colonisation and catheter related bloodstream infection (CRBSI) was recorded.
Results: Three hundred and four single lumen study catheters were inserted into 268 patients. Total duration of catheterisation was 5449 days (median, 12 days/catheter). Complete data could be evaluated in 270 catheters: 128 silver iontophoretic catheters and 140 untreated catheters. Forty seven silver iontophoretic catheters (36.7%) were colonised compared with 48 control catheters (33.8%). Seven cases (5.5%) of CRBSI occurred in patients who received silver iontophoretic catheters, compared with 11 cases (7.7%) in patients receiving control catheters. There was no significant difference in the incidence of catheter colonisation or CRBSI between silver iontophoretic and control catheters. When the duration of catheter placement was taken into consideration, Kaplan-Meier analysis showed no significant difference in the risk of CRBSI between the silver iontophoretic catheters and the untreated catheters (p = 0.77).
Conclusion: There was no significant difference in the incidence of catheter colonisation or CRBSI among high risk patients between silver iontophoretic catheters and control catheters. Future prospective, randomised studies with a larger number of catheters are encouraged to confirm or refute these results.
- antiseptics
- catheter related bloodstream infection
- central venous catheter
- iontophoresis
- silver ions
- CFU, colony forming units
- CI, confidence interval
- CRBSI, catheter related bloodstream infection
Statistics from Altmetric.com
Infection associated with the use of central venous catheters is a major source of nosocomial infection in the hospital.1 Catheter related bloodstream infection (CRBSI) occurs when microorganisms gain access to the bloodstream via one of four routes: catheter hub contamination, catheter insertion site colonisation, contaminated infusate, and/or haematogenous seeding. The first two portals of entry are the most frequent routes via which CRBSI occurs.2–4
“Infection associated with the use of central venous catheters is a major source of nosocomial infection in the hospital”
Investigators have recently studied the protective effect of coating catheters with antibiotics or antiseptics in the prevention of catheter colonisation and CRBSI. Various combinations of antibiotics (such as cefazolin,5 rifampicin, and minocycline6–8) and antiseptics (silver sulfadiazine and chlorhexidine8,9) have been studied, with some coating limited to the external surface,8,9 and some including both internal and external surfaces.6–8 These catheters are primarily for short term use (the mean duration of catheterisation was 7.9 days), and the ability of these coated catheters to prevent CRBSI in longterm (exceeding 10 days) intravenous treatment had not been well studied.8 A novel catheter (OLIGON; Implemed, Boston, USA), which releases antiseptic (silver ions) in a controlled and sustained manner by an iontophoretic reaction, has been developed. We conducted a prospective, randomised trial to compare the effectiveness of these silver iontophoretic catheters with untreated catheters (ARROW; Arrow International, Reading, Pennsylvania, USA) in reducing the incidence of catheter colonisation and CRBSI. The aim of our study was to test the null hypothesis that there was no difference in the incidence of catheter colonisation and CRBSI between the two treatment groups.
PATIENTS AND METHODS
Study population
All patients who required central venous access over a period greater than seven days were eligible to participate in our study. Most patients in our study required central venous access for total parenteral nutrition. Patients were excluded if they were younger than 18 years of age, had a history of allergy to silver, needed multilumen central venous access, or were pregnant. Our study was approved by the hospital ethics committee and written consent was obtained from each patient before entering into the trial.
Study catheter materials
Patients were randomly assigned to receive 7 French, 16 cm long, single lumen, silver impregnated polyurethane catheters (treatment group) or 7 French, 20 cm long, single lumen polyurethane catheters (control group). According to the manufacturer’s information, silver ions, in addition to carbon and platinum particles, are impregnated into the structure of the OLIGON polyurethane catheters. The silver particles interact with fluid in the body or infusate, which results in a sustained release of silver ions into the fluid–catheter interface. The movement of electrons from silver to platinum particles balances this chemical reaction. Only very small amounts of silver ions are released, but they are sufficient to cause a local antiseptic effect at the catheter–fluid interface.
Pilot study
Because the silver iontophoretic catheter is a new development, no clinical data exist in the literature. Therefore, we performed a pilot study to determine any potential problems in methodology and data collection, and to obtain preliminary estimates for the planning of the full analysis. In this study, patients were randomly assigned to receive either the treatment or control catheters. The randomisation codes were generated by computer and were concealed in separate envelopes, which were opened sequentially after the patients had enrolled in the trial. We set an initial study population of 50 catheters.
Full study design
After the pilot study, we discovered that some patients with concurrent sepsis were assigned into a particular study group. These patients were at high risk of further catheter related infection and could potentially skew the outcome of our study. Therefore, for the full study, we decided to stratify the patients into two subgroups—high and low risk—before randomisation. The stratification criteria were based on systemic inflammatory response syndrome criteria10 at the time of entry into our study. All patients with two or more criteria were stratified into the high risk group. Patients were then assigned the study catheters sequentially according to randomisation codes, which were concealed in separate envelopes. Randomisation was generated by computer in blocks of 10.
Central venous catheter insertion and maintenance
All central venous catheters were inserted aseptically by one person (JJB) into the subclavian vein. Providine iodine (Betadine; Adams Healthcare, Leeds, UK) was applied to the skin insertion site and surrounding area and allowed to dry. Large sterile drapes were placed around the insertion site and the catheters were inserted using the Seldinger technique. The practice of exchange of catheters over guidewire was not used. The catheters were secured with silk sutures and dressed with semipermeable transparent dressing. No antiseptic ointment was applied over the catheter insertion site. Infusion lines were changed every 48 hours by nurses and the dressings were changed once a week unless crumpled.
Catheters were only removed from the patients when intravenous treatment was no longer required or a complication, such as catheter leak, thrombophlebitis, insertion site infection, or CRBSI, had occurred. All the removed catheters were analysed in vitro by the roll plate11 and the endoluminal brush methods.12 Quantitative blood cultures (isolator lysis centrifugation system) were collected aseptically from a peripheral vein of those patients with suspected CRBSI. The quantity (colony forming units (CFU)) of organisms isolated from the peripheral blood culture was compared with that isolated from the endoluminal brush and luminal blood, and a differential colony count of 10/1 was suggestive of CRBSI.1 Recovered organisms were identified by standard microbiological methods (culture morphology, Gram stain, catalase and coagulase test, API (bioMerieux, Marcy, L’Etoile, France), etc) and by pulsed field electrophoresis to genotype organisms (coagulase negative staphylococci).
Definitions
Catheter colonisation was defined as the growth of 15 or more CFU in culture of the distal segment of catheter by the roll plate method11 or more than 100 CFU in cultures prepared by the endoluminal brushing technique.12 CRBSI was defined as the isolation of identical microorganisms (as identified by standard microbiology methods and pulsed field electrophoresis) from the colonised catheter and from the peripheral blood in a patient with clinical manifestations of sepsis.
Statistical calculations and analysis
Data from the two phases of our study, the pilot and the full study, were pooled and analysed on the intention to treat basis. Calculation of the sample size showed that a total of 180 catheters in each group would yield 80% power to detect a 5% absolute difference (10% to 5%) in the rate of CRBSI for each catheter among the patients randomly assigned to receive the treated or control catheters. The statistical differences between the two study groups were determined by the use of the Student’s t test or Mann-Whitney U rank sum test for continuous variables, and Fisher’s exact test or the χ2 test for categorical variables. All p values were based on two tailed tests for significance. The cumulative risks of developing CRBSI in the two groups as a function of the duration of catheterisation were estimated according to the Kaplan-Meier method and compared with the use of the log rank test. All statistics were analysed by using the SPSS 7.5 computer package; a p value < 0.05 was considered significant.
RESULTS
The trial was terminated prematurely because of difficulty in procuring silver iontophoretic catheters as a result of a technical problem outside our control—the bankruptcy of the manufacturer. A total of 304 study catheters (143 silver iontophoretic catheters and 161 untreated catheters) were inserted into 268 patients. The total duration of catheterisation was 5449 days (median, 12 days/catheter; mean, 17.9). Complete data could be evaluated in 270 catheters (89%): 128 silver iontophoretic catheters and 140 untreated catheters. The remaining 34 catheters (15 silver iontophoretic catheters and 19 untreated catheters) were not cultured (either being removed without notification or lost to follow up) and hence were excluded from our study. Table 1 shows the demographic data on both patients and catheters.
Demographic data on the patients and central venous catheters
Catheter colonisation
Forty seven of the 128 silver iontophoretic catheters (36.7%), compared with 48 of the 132 catheters (33.8%), were colonised according to at least one method of assessment (table 2).11,12 The difference between the two groups was not significant (relative risk, 1.01; 95% confidence interval (CI), 0.66 to 1.83; p = 0.72). When the duration of catheter placement was taken into account, Kaplan-Meier estimates of the risk of catheter colonisation showed no significant difference (p = 0.31 by the log rank test) between the silver iontophoretic catheters and the control catheters (fig 1). Median survival times were 11 and 14 days for the silver iontophoretic catheters and the control catheters, respectively. Table 3 shows the types of organisms isolated from the catheters by the use of the endoluminal brush or roll plate methods.
Incidence of catheter colonisation and catheter related bloodstream infection (CRBSI)
The organisms that colonised the silver iontophoretic and untreated control catheters
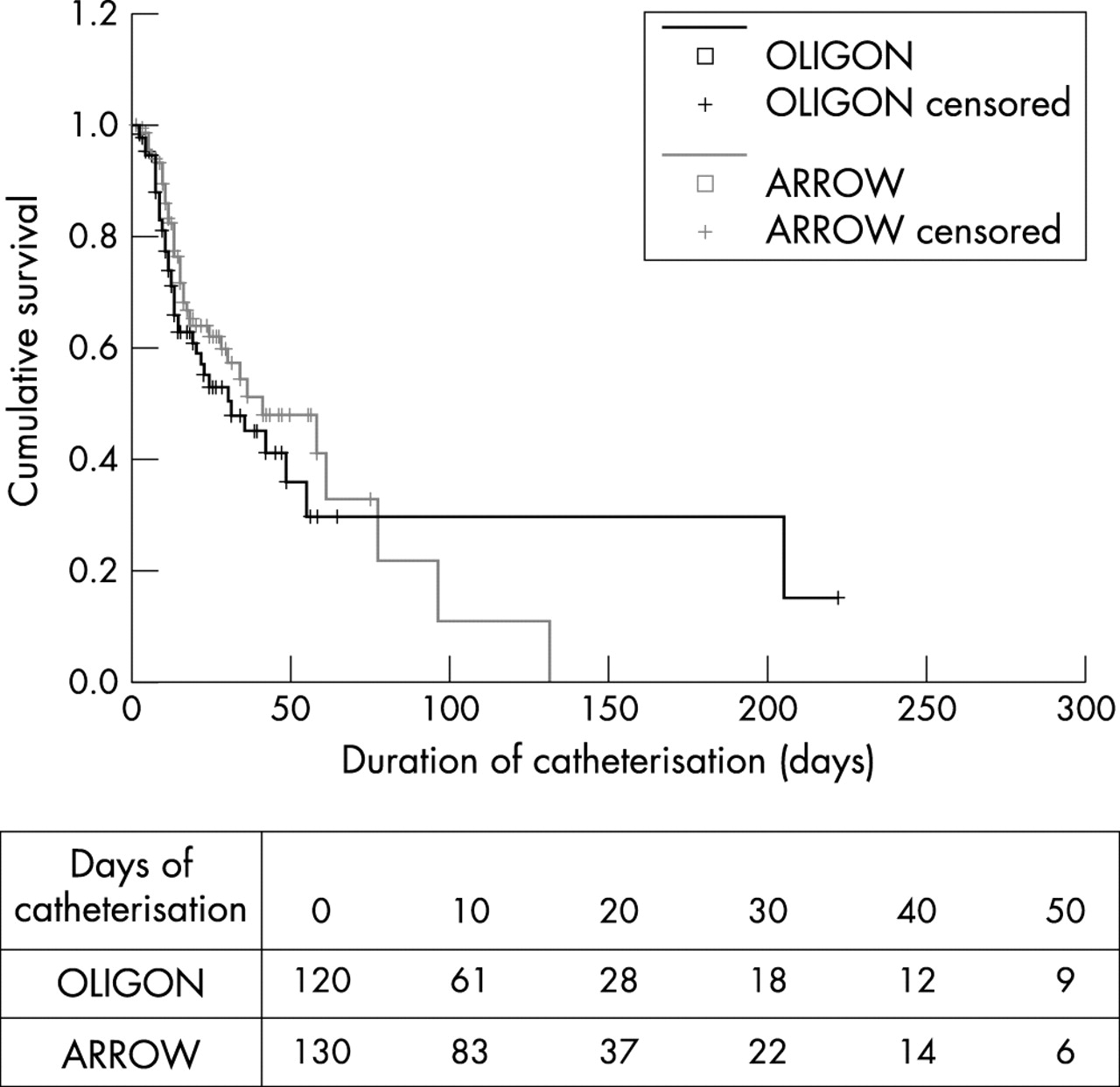
Kaplan-Meier curves for the cumulative survival of silver impregnated catheters and untreated catheters free from colonisation.
Catheter related bloodstream infection
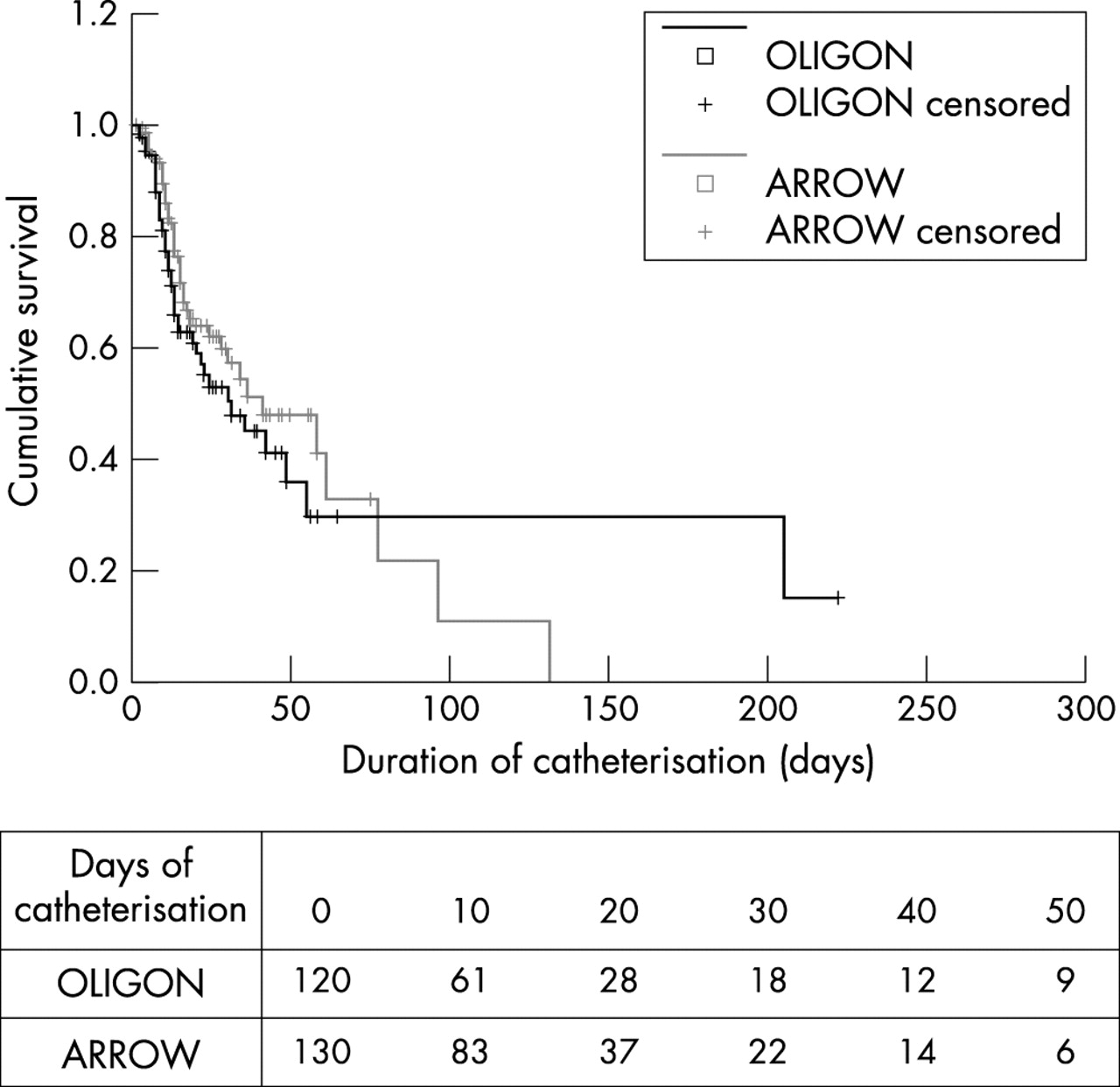
There were 18 cases (6.6%) of CRBSI. Seven cases (5.5%) of CRBSI occurred among the 128 silver iontophoretic catheters, compare with 11 cases (7.7%) of CRBSI among the 142 untreated catheters. There was no significant difference between the two study groups (relative risk, 0.71; 95% CI, 0.26 to 1.94; p = 0.51). The rates of CRBSI/1000 catheter days were 2.97 for silver iontophoretic catheters and 4.01 for the untreated catheters. Kaplan-Meier estimates of the risk of CRBSI according to the duration of catheter placement showed no significant difference in CRBSI rates between the silver iontophoretic and the control catheters (log rank test; p = 0.77) (fig 2). Analysis of the survival of catheters according to risk stratification revealed no significant difference between the low risk and the high risk groups in the two groups of catheters (low risk group, p = 0.33; high risk group, p = 0.68). Using the endoluminal brush method, significant endoluminal colonisation was detected in 12 cases (66%) (four silver iontophoretic and eight untreated catheters) of CRBSI, whereas significant extraluminal colonisation was detected in 13 cases (72%) of CRBSI (table 4).
Results of the endoluminal and extraluminal cultures on silver iontophoretic and untreated catheters associated with catheter related bloodstream infection

{kind=link}
{kind=link}
Kaplan-Meier curves for the cumulative survival of silver impregnated catheters and untreated catheters free from catheter related bloodstream infection.
DISCUSSION
CRBSI remains the most common complication associated with the delivery of total parenteral nutrition via the central venous catheter. Advances in biotechnology have allowed us to modify the catheter material (for example, from polyvinyl chloride to polyurethane) and to coat the surface(s) of the catheter with antiseptics (chlorhexidine and silver sulfadiazine8,9) and antibiotics (minocycline and rifampicin6–8) in an attempt to reduce CRBSI rates. Silver impregnated collagen cuffs can also significantly decrease the risk of short term catheter colonisation,13 although they fail to prevent longterm colonisation (J Groeger, A Lucas, A Brown. Silver-impregnated cuffs on Hickman catheters in cancer patients: a prospective randomised study of infectious morbidity. 29th ICAAC 1989, Washington DC. American Society for Microbiology, abstract 1079), possibly because of early degradation of the silver impregnated collagen cuff.
Many microorganisms carry a negative charge because of their cell wall components. Attempts have been made to apply a low voltage electrical current to repel bacteria from colonising the catheters. In an in vitro study, continuous direct current applied to a carbon impregnated catheter has been shown to be bactericidal against a range of microorganisms.14 A further development of this novel approach involves the impregnation of silver, platinum, and carbon particles into the polyurethane structure of the catheter (“OLIGON” or “Vantex” central venous catheter). This results in a continuous and sustained release of silver ions down the electrochemical gradient to the catheter surface, when the catheter material is placed in a conductive fluid medium (for example, saline, total parental nutrition, or blood). It has long been known that selected metals—such as gold, silver, and copper—have broad spectrum bactericidal and fungicidal activity, including activity against the common strains of organisms that cause device related infections. The most active form of these metals is in ionic solution,15–18 and silver is the most renowned and potent of all the oligodynamic metal ions. In the silver iontophoretic catheter, silver ions are released into the intraluminal and extraluminal surroundings. By controlling the component concentrations, particle sizes, aspect ratios, and processing parameters, different silver ion release profiles can be achieved. In vitro evidence suggests that silver ion release continues over a period of nine months (Implemed). There is good in vitro evidence of significant antimicrobial activity against Staphylococcus epidermidis, Staphylococcus aureus, Escherichia coli, Pseudomonas aeruginosa, Klebsiella pneumoniae, and Candida albicans (product information, Implemed). As far as we are aware, there are no clinical data published on the antimicrobial efficacy of this new catheter technology. In this prospective randomised controlled trial, we tested the antimicrobial efficacy of silver iontophoretic catheters, compared with control catheters made of the same material but without the silver impregnation.
From the outset, this study was designed to minimise many known confounding factors that are associated with a higher rate of CRBSI. Specifically, all the central venous catheters were inserted by a single person, placed in the subclavian vein, and received only total parenteral nutrition.
In our current trial, the 11% dropout rate compares favourably with other randomised control trials on antimicrobial catheters.6,7,9,18 We found that neither colonisation rates nor CRBSI rates were significantly better in silver iontophoretic catheters than in control catheters. In addition, the analysis of silver iontophoretic and control catheters on the basis of intention to treat showed no significance differences (data not presented) in the CRBSI rate. Further analysis of the high risk and low risk subgroups showed no significant differences in the colonisation or CRBSI rates, either with silver iontophoretic or untreated catheters.
Take home messages
-
There was no significant difference in the incidence of catheter colonisation or catheter related bloodstream infection among high risk patients between silver iontophoretic catheters and control catheters
-
Future prospective, randomised studies with a larger number of catheters should be undertaken to confirm these results
“The fact that the difference in infection rates between these two types of catheters was not large suggested that the clinical impact of silver iontophoretic catheters would not be clinically significant”
We were able to assess independently microbial colonisation in both the inner and outer surfaces of the catheter by using the roll plate or endoluminal brush methods. Endoluminal colonisation was associated with 71% cases of CRBSI and a similar percentage also had concurrent extraluminal colonisation on the catheter tips. Therefore, endoluminal and extraluminal infection appears to be equally important in the pathogenesis of CRBSI in our series. Neither of the two types of study catheters was better than the other at preventing colonisation in either the external or internal surface of the catheters.
No toxic effects of the silver ions, such as argyria (blue-grey discolouration of skin), kidney failure, or liver necrosis, were encountered in our study. According to the manufacturer’s information, no adverse effect would be expected even if more than two catheters were in place continuously from birth through to the age of 60.
The main criticism of our study is that the failure of silver iontophoretic catheters to reduce colonisation or CRBSI rates may represent a type II error that could by eliminated by a larger study size. However, the fact that the difference in infection rates between these two types of catheters was not large suggested that the clinical impact of silver iontophoretic catheters would not be clinically significant.
In conclusion, our study found no significant reduction of colonisation or CRBSI rates when silver iontophoretic catheters were used compared with standard untreated polyurethane catheters. Further large prospective, randomised controlled trials are required to confirm these results.
Acknowledgments
This study was supported in part by Implemed Inc, Boston, USA.