Article Text

Abstract
Background: Airway narrowing in acute bronchiolitis does not respond to inhaled bronchodilators but does to adrenaline when compared to bronchodilators. Influences of supportive care were not considered in previous treatment studies.
Methods: Short term effects of nebulised adrenaline and saline placebo were compared in infants with moderately severe acute bronchiolitis. Thirty eight infants were recruited, 19 in each treatment group. After stabilisation, infants received a single 3 ml dose of either levo-adrenaline (3 mg) or 0.9% saline placebo via Pari-BABY nebuliser driven with 6 l/min oxygen for three minutes. Changes in respiratory rate (RR), heart rate (HR), oxygen saturation (Spo2), Respiratory Distress Assessment Instrument (RDAI), and activity levels were assessed at 20 minutes intervals at times −20, 0, 20, 40, and 60 minutes around treatment. Respiratory virology and chest x ray were performed.
Results: Supportive therapy prior to study treatment resulted in significant reductions in RR (by 4.3 breaths/min) and HR (by 4.6 beats/min); there were no changes in Spo2 or RDAI. There were no further changes in any parameter in either treatment group at any assessment time after treatment.
Conclusion: No improvement was shown with inhaled adrenaline in acute bronchiolitis, when compared with supportive care or placebo. Improvements noted pretreatment question whether prior noted improvements were through supportive care or pharmacological interventions.
- acute bronchiolitis
- nebulised
- epinephrine
- adrenaline
- bronchodilator
- wheezy infant
Statistics from Altmetric.com
A cute bronchiolitis is commonly a cause for admission to hospital in infants during winter. Current management is supportive, utilising fluids and oxygen, with no specific therapy to influence the natural history or progression of the disease.1
Affected infants become increasingly dyspnoeic and hypoxic for three to four days, after which most improve spontaneously.2 During the convalescent phase, respiratory secretions and debris become thicker and more abundant, occasionally blocking lower airways with segmental atelectasis in severe case. Although the hallmark of bronchiolitis is airway narrowing, this has been shown to be unresponsive to bronchodilator therapy,3–6 including specifically the airway blockage that characterises the recovery phase.7
Adrenaline has a number of advantages over β2 adrenergic selective bronchodilators that ensure its efficacy with fewer side effects: (1) α adrenergic vasoconstrictor action that can decongest the mucosa, limit its own absorption, and regulate pulmonary blood flow, with little effect on ventilation–perfusion matching; (2) β2 adrenergic bronchial muscle relaxant effect; (3) β2 adrenergic action to suppress release of chemical mediators; (4) physiological antihistamine effect that can reverse histamine effects, such as oedema; and (5) it reduces catarrhal secretions.8
β2 Adrenergic bronchodilators have mucosal and pulmonary vasodilator effects. The former increase mucosal absorption rates with resultant direct tachycardic effects, by virtue of the residual inherent β1 adrenergic activity effects. The latter enhance ventilation–perfusion mismatching which results in hypoxia and hypoxia induced tachyarrhythmia. Airway obstruction increases work of breathing and precipitates hypoxia; both are associated with tachycardia. The vasoconstrictor and bronchodilator activities of adrenaline protect against its direct as well as hypoxia induced arrhythmogenicity. It is therefore not surprising that in clinical studies, drugs such as salbutamol, with minimal residual β1 adrenergic activity, have more potential to cause tachycardia than adrenaline, which in spite of its potent β1 adrenergic activity might reduce heart rate.1,9
Many recent studies have reported on the efficacy of inhaled adrenaline (epinephrine) in the treatment of bronchiolitis, but were subject to criticism over patient selection10–12 and study design,9,12–13 in particular the use of bronchodilators for comparison. In this study, with continued standard supportive care, we compared the efficacy and safety of nebulised adrenaline against saline as placebo in infants less than 1 year of age presenting with moderately severe acute bronchiolitis.
PATIENTS AND METHODS
Patients
We studied infants aged 30 days to 1 year within the first four days of their respiratory illness who had clinically, rather than virologically diagnosed bronchiolitis, as defined by Court,14 of sufficient severity that oxygen therapy was required to keep saturations ≥94% or with tachypnoea of ≥50 breaths/min. Patients were studied at presentation to hospital, having been referred by their general practitioners to our paediatric assessment and admission unit. Infants were not eligible if the disease duration was greater than four days, as we were interested in studying responsiveness during the progressive phase of the disease. Thereafter mucoid secretions assume a more important role in airway blockage at the convalescent stage. Subjects were further excluded if they had a history of a previous wheezy episode, or chronic lung, cardiac, or neuromuscular disease. In addition, recruitment was delayed for 24 hours if the infant had received oral steroids, or for 2 hours if they had received inhaled bronchodilators.
Intervention
The infants were stabilised with antipyretics if necessary (temperature >38°C) and/or nasal suction if the nose was blocked. Facial oxygen was removed if the oxygen saturation (Spo2) was >90% in air; if not, it was provided to maintain Spo2 at 90–92%. This situation was maintained for at least 30 minutes before the patients received any study treatment and was left unaltered throughout the study. After stabilisation, the infants received minimal handling to allow them to settle or sleep.
Infants were studied in a double blind placebo controlled manner with randomisation in balanced blocks of eight. The infants were randomised to a single dose (3 ml) of either levo-adrenaline (3 mg), the commonly available form in the UK, or 0.9% saline placebo. Treatment was nebulised in 100% oxygen at 6 l/min for three minutes using a Pari-baby nebuliser and soft silicon rounded facemask held gently to make a tight seal around the nose and the mouth. The adrenaline dose is based on the maximum dose used in a previous study.9 We chose a single large dose of 3 mg in preference to repeated smaller doses, as is the practice in the treatment of croup, to avoid repeated change in activity status. We considered that frequent handling of these infants might invalidate the study, should discrepancy within subjects or between groups become considerable.
Assessment
The infants were assessed five times: twice before treatment (times −20 minutes and zero), and three times thereafter, at 20, 40, and 60 minutes. Assessments prior to treatment evaluated changes with supportive therapy and stabilisation alone.
Assessments at each point were:
Respiratory rate: counted manually, by both palpation and visual observation of chest excursion, for a complete minute on two occasions; average recorded.
Heart rate: taken from pulse oximeter reading five times during a one minute period; average of five readings recorded.
Spo2: taken from pulse oximeter reading five times during a one minute period; average of five readings recorded.
Respiratory clinical status was assessed using the Respiratory Distress Assessment Instrument (RDAI) developed by Lowell and colleagues.10
The infant's status of activity (four levels: asleep, quiet, agitated, and crying) during assessments was documented.
To study the safety of nebulised adrenaline, all subjects were admitted at least for a day, even though many were expected to improve and to be ready for discharge. The aim was to observe adequately for adverse effects such as vomiting, pallor, tremor, or arrhythmia.
Informed consent was obtained from parents. The local ethics committee approved the study.
Sample size
As an assessment of treatment efficacy, a reduction in respiratory rate of 7 breaths/min was regarded as important. Assuming a standard deviation of the respiratory rate of 7 breaths/min, with an α error of 0.05 (two tailed test) and power of 90%, a sample size of 21 infants per group would be sufficient to detect an important treatment effect.
As an assessment of treatment safety, an increase in heart rate by 15 beats/min was considered important. Assuming a standard deviation of the heart rate of 15 beats/min, an α error of 0.05 (two tailed test) and power of 90%, a sample size of 21 infants per group would be sufficient
Primary outcome measure was the changes in respiratory and heart rates, as compared between the groups, before any nebulised treatment and 20 minutes after either saline or adrenaline nebulisation.
Statistical analysis
Statistical analysis used the Statistical Package for Social Sciences, version 10. The investigator and statistician were blinded to treatment allocation, with treatment groups labelled groups 1 and 2. Non-parametric data were analysed using Pearson's χ2, Fisher's exact test, or the Mann–Whitney test; parametric data were analysed using the paired t test and general linear model for repeated measurements analyses.
RESULTS
The study period was from mid December 1998 to the end of May 2000 and thereby encompassed two winters. All infants admitted to the Leicester Royal Infirmary Children's Hospital during this time with a clinical diagnosis of bronchiolitis, who were thought to be suitable for study, were referred for assessment.
We assessed 109 infants and recruited 38 (35%) into the study. The remaining 71 were not recruited, either through failure to obtain parental consent (n = 22) or ineligibility (n = 49). Reasons for rejection were: disease too mild (n = 21), recurrent wheeze (n = 9), symptoms more than four days duration (n = 9), recent systemic steroids (n = 4), lobar collapse (n = 2), mechanical ventilation required (n = 2), neurological disease (n = 1), and chronic lung disease (n = 1).
The two treatment groups were similar for age, gender, respiratory virology, radiology, and clinical signs at baseline assessment (table 1).
Baseline assessments
Although activity status changed in some infants as a result of nebulisation, it generally returned to the prenebulisation state by the time of the first post-nebulisation assessment (at 20 minutes). Therefore, during the study period the activity status was on average similar between groups, excluding its influence on the five points of assessments (χ2 = 0.44, 0.69, 0.92, 0.26, and 0.94); for example, a decrease in activity might decrease an infant's heart rate.
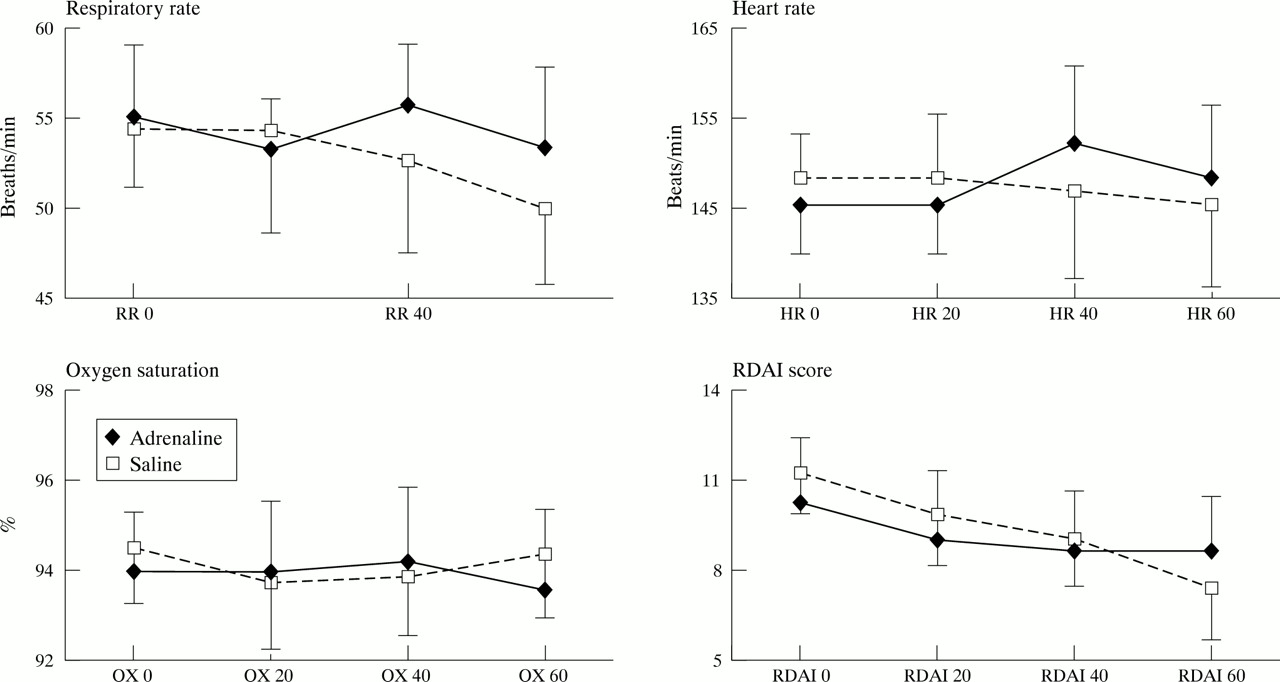
Stabilisation and pretreatment supportive care resulted in significant falls from baseline in both respiratory rate (mean (95% CI) 4.3 (1.6 to 7); p = 0.003) and heart rate (mean (95% CI) 4.6 (0.4 to 8.8); p = 0.031); Spo2 and RDAI were unchanged. These were the only significant changes observed throughout the study. In the saline group, heart rate tended to fall very slowly over time. In the adrenaline group, it remained at the same level at 20 minutes, then increased by a mean of 6.7 beats/min at 40 minutes, signalling a mild statistically insignificant tachycardia (p = 0.315). This did not last for long, as at 60 minutes it was almost back to baseline levels (fig 1).
{kind=link}
Mean (95% CI) for respiratory rate, heart rate, oxygen saturation, and RDAI score for infants in each group at 0, 20, 40, and 60 minutes of assessment.
The average changes noted between treatment groups in cardiorespiratory parameters, with initiation of treatment as assessed at 20, 40, or 60 minutes, were not statistically significant (fig 1). Furthermore, when these changes were non-parametrically-assessed in individual cases among the groups, they were not significant. No side effects were noted in either group.
DISCUSSION
In this study nebulisation with adrenaline had no beneficial or deleterious effect on the cardiorespiratory status of infants with acute, moderately severe bronchiolitis. However, supportive or nursing care (reduction of a high temperature, clearing blocked nostrils in these obligate nose breathers, feeding a hungry infant, changing a wet nappy, and observation with minimal handling) did result in significant reductions in both respiratory and heart rates. This component of care was not assessed in previous studies.9–13
The mechanisms by which adrenaline might increase airway calibre in bronchiolitis are through bronchodilatation by β2 sympathomimetic activity, reversal of tissue oedema through vasoconstriction by α1 actions, and a physiological antihistamine effect which ensures mucosal decongestion.1 Saline is thought to produce its placebo effects by liquefying dry secretions, assisting their clearance, and by humidifying and soothing injured mucosal surfaces, hence reducing irritation.
This study emphasises two important methodological issues when investigating an acute illness that will improve spontaneously with time. Firstly, to assess the effect of supporting and observing the child, a treatment modality which is well established in bronchiolitis; and secondly, to compare the study treatment to its vehicle as the vehicle itself may be beneficial. Previous studies compared adrenaline with salbutamol and failed to account for the effects of supportive care and improvement with time.1,9,13
A possible criticism of this study might be the failure to recruit the projected number of subjects into each treatment arm. However, although the study was short of two patients per treatment arm, the amount of overlap in confidence intervals made this shortfall statistically insignificant and thereby negated the possibility of missed differences.
A further criticism might be the insufficiency of the delivered adrenaline dose. Although we used the highest dose, 3 mg, reported in such studies, an increase in heart rate by 6.7 beats/min on average was noted in the treatment group at 40 minutes; this had resolved by 60 minutes. This suggests that the small range of aerosol particle size produced by the Pari-BABY nebuliser ensured minimal oropharyngeal deposition and absorption, while lung deposition occurred. The α adrenergic activity of adrenaline ensured local respiratory tract vasoconstriction and delayed its own systemic absorption. This is the main reason for choosing: (a) the Pari-BABY nebuliser, to minimise side effects by eliminating non-targeted organ absorption (upper respiratory tract); (b) the mucosal vasoconstrictor adrenaline (rather than the vasodilator salbutamol), which limits its own absorption and hence its direct cardiac effects; and (c) the pulmonary vasoconstrictor adrenaline, which does not induce perfusion–ventilation mismatching and hypoxia, which has an indirect arrhythmogenic potential.
Nebulised adrenaline cannot be recommended as treatment for infants with a moderately severe first attack of bronchiolitis on the results of this study. However, as it was found non-deleterious to patients it might be considered for its bronchodilator properties in infants over 1 year of age with recurrent wheeze.
Acknowledgments
We thank Professor Michael Silverman (University of Leicester), for his constructive criticism and advice throughout the study; the staff of the respiratory ward at Leicester Royal Children's Hospital; Mr Derek Bainbridge (PARI Medical Ltd), for providing the nebuliser devices used in this study; Dr Ali A Sadiq (Alexandria University) for statistical advice and reviewing the manuscript; and Mr Bradley Manktelow for reviewing the final statistical results.